
POCUS for Vascular Access Small Group Clinic
Choosing the Right Access
Q = (π × ΔP × r⁴) / (8 × η × L)
Flow depends on radius⁴ and inversely on length
| Device | Typical Size / Length | Flow Reality | Dwell Time | Use Case |
|---|---|---|---|---|
| Short PIV | 14–20G, 3–5 cm | ~60–200+ mL/min depending on gauge; short length allows high flow | Days | Routine access; can be resuscitative if large bore |
| Midline | 18–22G, 8–20 cm | Longer length reduces flow vs PIV of same gauge; power injection up to ~5–7 mL/s | 2–4 weeks | DIVA, longer therapy, non-vesicants |
| RIC | 7–8.5 Fr, ~5–6 cm | Very high flow (~1 L/min) | Hours | Resuscitation, massive transfusion |
| Micropuncture | 21G → upsized | Depends on final catheter placed | N/A (technique) | DIVA rescue → upsizing |
Take Away: Short + wide = fast. Long = slower (even if gauge is the same).
PIV = peripheral IV, RIC = rapid infusion catheter, DIVA = difficult vascular access
Midline Catheters
What is a midline?
Peripheral catheter placed in upper arm veins
Tip terminates proximal to axilla (not central)
Dwell time: 2–4 weeks
Indications:
DIVA
Need for IV therapy > 5–7 days
Frequent blood draws
Non-vesicant medications
Contraindications:
Vesicants (usually continuous, short courses or single doses may be tolerable but weigh risks/benefits).
TPN
Need for central access (e.g., multiple pressors, hyperosmolar infusions)
Local infection / upper extremity DVT
Risks:
Extravasation
Thrombosis (↑ brachial vein)
Nerve Injury
Arterial Cannulation
Placement:
Mid-arm, avoid close to antecubital fossa → can cause elbow triangle ecchymosis
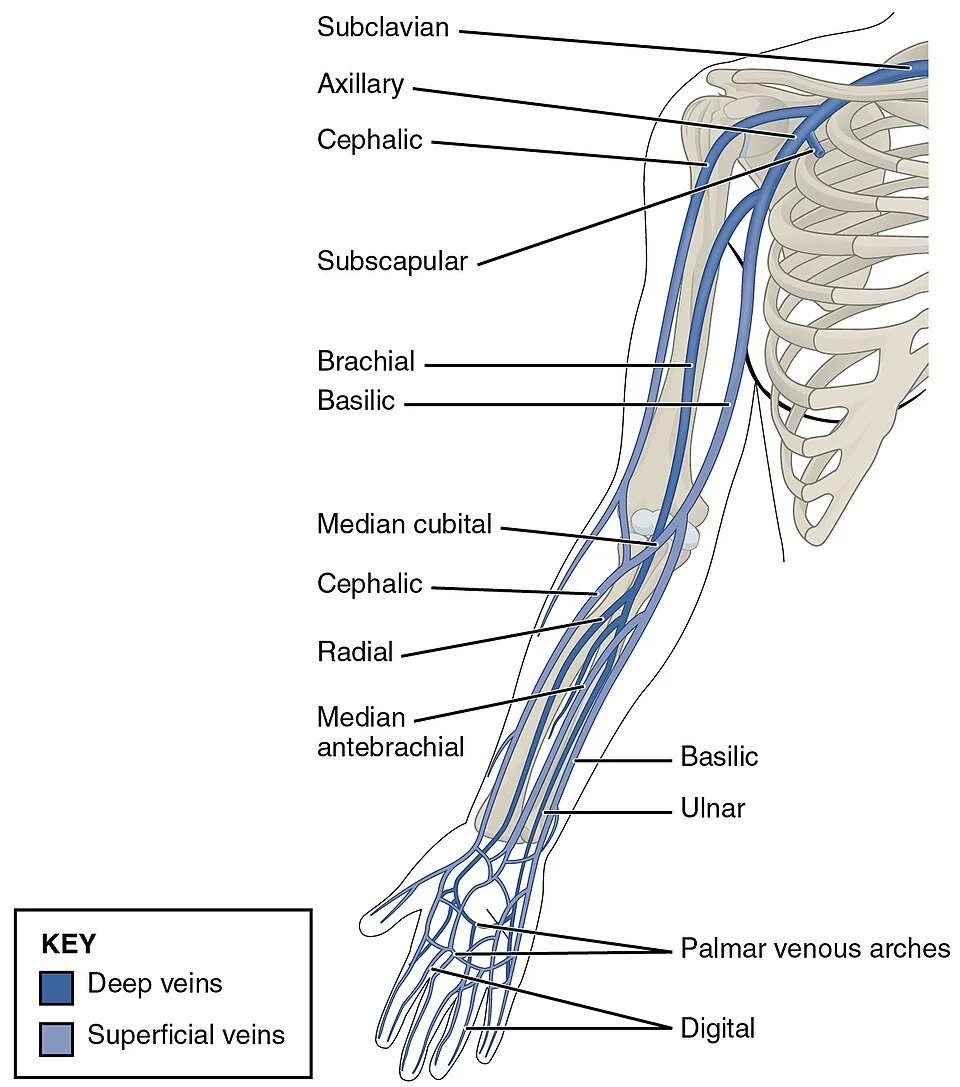
Basilic vein preferred. Cephalic vein tapers distally, may not be ideal placement.
Brachial vein — high risk of thrombosis.
Distal placement near the antecubital fossa is associated with increased mechanical complications, often seen clinically as bruising, bleeding, and early line failure.
High motion zone (flexion/extension)
Leads to:
Line kinking
Dislodgement
Bleeding
Dressing failure
Extravasation
Single Lumen
Most common
Lower thrombosis risk
May be less stable (softer catheter)
Double Lumen
Allows simultaneous infusions
Higher thrombosis risk (more catheter bulk → ↓ vein-to-catheter ratio)
Requires:
Larger insertion tract
Often dilation
More procedural time
Rapid Infusion Catheters (RICs)
What is a RIC?
Large-bore peripheral catheter (~7–8.5 Fr, ~5–6 cm)
Placed using Seldinger technique (often over existing PIV, can be done after micropuncture)
Designed for rapid, high-volume infusion
Indications
Trauma / hemorrhage
Massive transfusion
Septic shock
Any high-flow need
DIVA when PIV placement fails
Pros
Very high flow rates (superior to standard PIVs)
Faster than placing central line in emergent settings
Fully peripheral → avoids central line complications
Can be placed rapidly in experienced hands
Cons
Short-term use only (resuscitation device)
Requires procedural skill (wire + dilation)
Not suitable for:
Vesicants
Long-term therapy
Placement
Upper arm veins preferred (basilic > cephalic > brachial)
Large, straight vein segment
Avoid:
Small distal veins
Areas crossing joints
Complications
Mechanical
Vessel injury during dilation
Hematoma
Failed upsizing
Leaving dilator in place — do not forget to remove dilator
Infusion-related
Extravasation
Compartment syndrome (rare but serious)
Tissue ischemia / necrosis (high-pressure infusions)
Risk increases with:
High flow rates
Poor vein selection
Catheter malposition
Other
Thrombosis
Infection (lower than central lines but still possible)
Micropuncture Kit
What is a micropuncture kit?
Small-caliber access system:
21G needle
0.018″ wire
4–5 Fr sheath
Uses Seldinger technique for stepwise access
Indications
DIVA
Deep or small veins
Failed standard PIV attempts
Need for:
RIC placement
Midline placement
Can realistically be used for any Seldinger procedure (eg, pericardiocentesis)
Why It Works
Smaller needle → less vessel trauma
Wire access → confirms intravascular placement
Stepwise dilation → controlled upsizing
Placement
Target:
Vein diameter ≥ ~4 mm
Straight segment of vein
Prefer upper arm veins for upsizing
Avoid placement near joints
Complications
Inadvertent arterial puncture during venous access
Hematoma
Wire misplacement
Vessel injury (rare)