General notes —
Must be in abdominal setting or aorta setting if available.
Must visualize the spinal body as a landmark in general for the aorta. If the spinal body is not visualized erroneous interpretation is likely to occur due to evaluating a different vessel. A common error is to assume the SMA is the aorta.
Keep the aorta within 2/3rd of the screen, do not have excess zoom or excess depth. The probe should ideally be perfectly perpendicular to the body when measuring.
Bowel gas may be moved out of the way using graded compression.
Start proximally at the celiac trunk (if able to visualize) and proceed distally to the bifurcation of the iliac vessels.
It is not always possible to visualize the celiac trunk so if you do not, keep moving on. Most aneurysm are infrarenal (~85%) and thus below the level of the SMA.
Measure the aorta at the proximal aorta, mid aorta, distal aorta, and both iliac vessels if able.
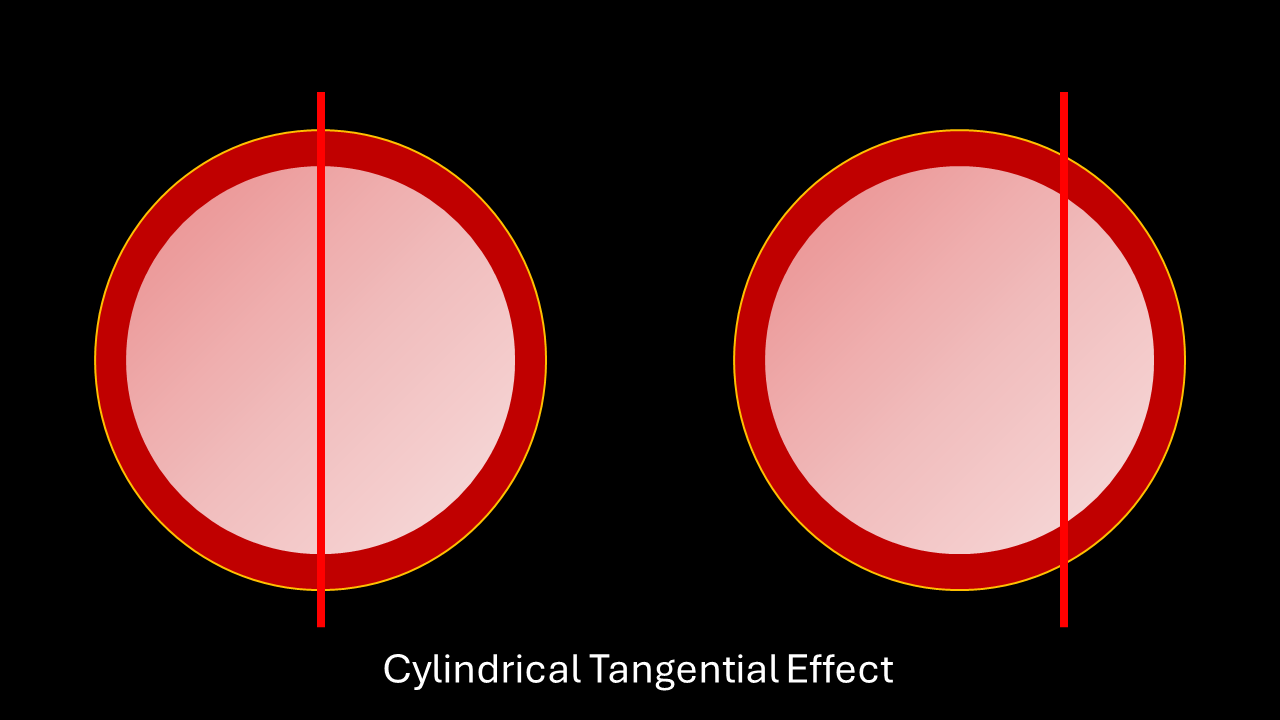
Obtain a longitudinal view of the aorta to evaluate for saccular aneurysms. Ideally, do not measure longitudinally due to the cylindrical tangential effect.
If an abdominal aortic aneurysm (AAA) is visualized continue to scan the entire aorta if possible, both for completeness and to evaluate the extent of the aneurysm.
Proximal aorta —
Anatomical land mark: celiac trunk. Appears as a “sea-gull” sign.
Branches into the common hepatic artery and splenic artery.
Mid aorta —
Anatomical landmark: superior mesenteric artery. Appears as a “pie-in-the-sky” or “mantle clock.”
Most AAA’s are infrarenal. The SMA is a landmark for the renal arteries (which may or may not be visualized).
Distal aorta —
Visualize the bifurcation of the iliac vessels and move just proximally to obtain the distal aorta, measure.
Bifurcation of the iliac vessels —
Visualize both iliac vessels and measure. They should measure under 1.5cm.
Longitudinal view of the aorta —
Obtain a longitudinal view of the aorta to evaluate for saccular aneurysms.
In generally the widest portion may be measured for the A-P diameter of the aorta, however due to the cylindrical tangential effect it is acceptable to not measure the aorta in the longitudinal view for POCUS unless a saccular aneurysm is noted.
Cylindrical tangential effect — measurements in the longitudinal view may not cut through exactly though the center of the aorta or the largest portion, may be incorrectly measured.