
POCUS Thoracic
General notes —
When evaluating for pneumothorax any probe can be used as long as depth is reduced significantly. A high frequency linear probe maybe slightly faster at detecting a pneumothorax, but the difference is inconsequential.
Start at the anterior of the chest at the apices and evaluate multiple rib spaces.
Lung ultrasound is a highly sensitive modality to detect a pneumothorax.
Compared to supine CXR, US was more sensitive.
Evaluate for lung sliding —
First evaluate for lung sliding.
Lung sliding occurs due to the interface between the visceral and parietal pleura of the lung. This is characterized as the classic shimmering, or “ants-marching” along.
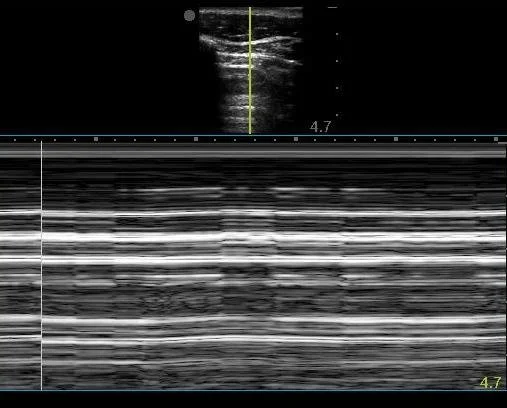
On M-mode this appears as a “sandy-beach,” or “sea shore” sign.
The presence of lung sliding effectively rules out pneumothorax at the point being examined.
B-lines have a high negative predictive value as well, and seeing B-lines also effectively rules out pneumothorax at the point being examined.
Note the Lichtenstein paper calls B-lines “comet-tail artifacts.” Comet-tail artifacts are distinct from B-lines in that one is a short path reverberation artifact while B-lines are a ring-down artifact, but some older papers still use them interchangeably.
True comet-tail artifacts also require a parietal-visceral interface and effectively rule out pneumothorax.
Absent lung sliding —
Absent lung sliding is a sign that there may be a pneumothorax.
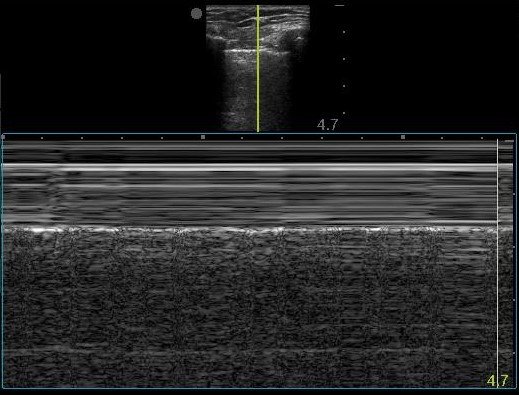
On M-mode may appear as “bar-code” sign, or sometimes known as “stratosphere sign.”
Absent lung sliding is a sensitive finding for pneumothorax; however it is not specific and may occur due to a number of other pathologies.
Evaluate for lung point —
Lung point indicates the transition point between the pneumothorax and normal contact between the visceral and parietal pleura begins.
Lung point may be found by moving the the transducer laterally to find the location where the visceral pleura loses contact with the chest wall.
Lung point may not be seen in massive or complete pneumothorax.
Lung point is purportedly 100% specific for pneumothorax, however this is likely slightly exaggerated.
There are very few false positives for lung point —
Bleb-point — large blebs where lung tissue disappears completely below the pleura may create a lung point mimic.
Pseudo-lung point — present at the border of contused lung and well aerated lung.
Pleural adhesions — diseased lung causing adhesions may not demonstrate lung sliding and the transition point may mimic lung point.
In the vast majority of cases, the absence of lung sliding with a discovered lung point is a pneumothorax.