
General notes —
Must be in abdominal setting (do not use cardiac settings).
At least two views, long and short should be obtained with fan through clips.
Measurement of the anterior gallbladder wall thickness.
Look for the six signs of cholecystitis:
Anterior gallbladder wall (AGBW) thickening ≥4mm
Gallbladder wall edema
Hydropic gallbladder (10cm x 5cm)
Stone-in-neck (SIN) sign
Pericholecystic fluid
Sonographic Murphy’s
Aside from the SIN sign, there is no requirement for gallstones to be present to diagnose cholecystitis (eg, acalculous cholecystitis).
Measure common bile duct diameter. If LFTs and lipase are normal and there are no signs of cholecystitis, not always necessary.
Identifying the gallbladder —
Start from medial approach or the lateral approach tracing the liver edge.
Can use intercostal or subcostal windows.
Can use color or power doppler to identify vascular structures.
The gallbladder has no doppler signal and is often the most anterior structure in the right upper quadrant.
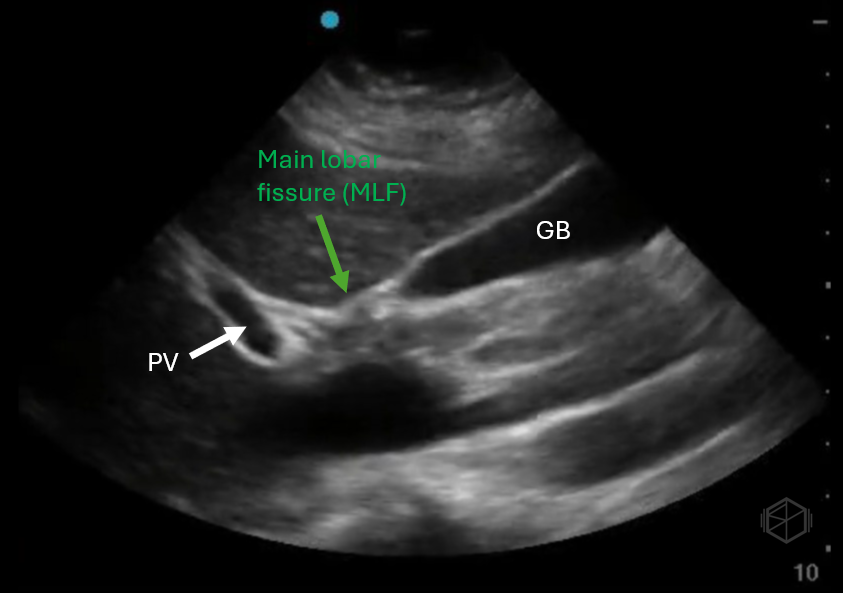
Anatomical land mark — main lobar fissure.
Found in about 70% of people, the MLF is a hyperechoic landmark connecting the portal triad to the gallbladder.
MLF is a reliable landmark to locate the gallbladder.
Signs of acute cholecystitis
AGBW thickening ( ≥4mm)
Measure the AGBW to avoid posterior acoustic enhancement leading to a false measurement.
Classically >3mm is considered thick, however ≥4mm is more specific without much loss in sensitivity.
May be present with or without gallbladder wall edema.
Can be measured in either long or short.
If there is focal wall thickening, make multiple measurements.
Similar to gallbladder wall edema, there may be both intrinisc and extrinsic causes of AGBW thickening.
Thickened gallbladder wall
GB wall thickening, mild
Gallbladder wall edema
Gallbladder wall edema is a non-specific finding that may occur in a multitude of pathologies.
Slightly different than thickening on it’s own. Gallbladder wall edema is the development of fluid within the gallbladder wall.
The mechanism for developing edema that is not due to lithiasis is not well known but suspected to occur due to elevated portal venous pressure, increased systemic venous pressure, decreased osmotic intravascular pressure, increased vascular permeability, or any combination of these.
It can be sign of acute or chronic cholecystitis, however it can be present in:
Liver pathologies including: cirrhosis, hepatitis
Generalized edematous states: congestive heart failure, hypoalbuminemia, nephrotic syndrome
Ascites
Extra-cholecystic inflammation: pancreatitis, pyelonephritis, peritonitis, perforated duodenal ulcers
Some viral infections: mononucleosis, dengue, HIV/AIDS
Malignancy / gallbladder carcinoma
Gallbladder wall edema from acute cholecystitis, patient had positive sonographic Murphy's.
Diffuse gallbladder wall from CHF
Diffuse gallbladder wall edema from cirrhosis with ascites
Hydropic gallbladder (≥10cm x 5cm)
A hydropic gallbladder (in adults) is one that measures over 10x5cm.
A wider gallbladder (>5cm) is considered worse than an elongated one and portends a higher complication rate such as necrosis.
Gallbladder hydrops usually occurs due to poor drainage of the gallbladder often caused by an obstructing stone near the cystic duct (but can occur for a number of other reasons including malignancy, cystic fibrosis, Kawasaki disease, ascariasis etc.). Bile reabsorption occurs slowly and the gallbladder wall releases mucoid or clear content which leads to distention. True hydrops occurs when the gallbladder distends without signs of inflammation.
Significantly hydropic gallbladder filled with sludge and stones.
Significantly elongated gallbladder, acutely inflamed gallbladder with hydrops operatively.
Significantly hydropic gallbladder with multiple other signs of cholecystitis.
Stone-in-Neck sign
Impacted stone in the neck of the gallbladder — specific (97%) to cholecystitis with a high positive predictive value (94%), even in the absence of other signs of cholecystitis.
True SIN sign is defined as the lack of an anechoic space between the gallbladder neck and the immobile stone it contains without other ultrasonographic evidence of cholecystitis.
Must image the gallbladder neck to avoid missing this sign.
Pericholecystic fluid
Pericholecystic fluid is not very common and it has a low sensitivity, but when it is present is highly specific for cholecystitis with a high likelihood ratio.
Fluid, in general, makes sharp angles, look for anechoic or hypoechoic sharp angles.
Sonographic Murphy’s
Assessed by compressing with the probe directly over the gallbladder in the subcostal view.
Will not work through the intercostal view as this is compressing over the ribs.
A positive sonographic Murphy’s is when the point of maximal tenderness is directly over the gallbladder. May also be noted as an abrupt cessation of inspiration with the probe over the gallbladder although this is not necessary.
Analgesia should not mask this sign; however, there is still suspicion that it might lead to false negatives. (19584736, 15837021)
Classically, the presence of stones + a Sonographic murphy’s sign has a 92.2% PPV for acute cholecystitis. Add in AGBW thickening and that becomes 95.2% (3890007).