
POCUS Echocardiography
General notes —
Tamponade is a clinical diagnosis.
Consider Beck’s triad: hypotension, jugular venous distention, and muffled heart sounds.
POCUS signs precede clinical tamponade and POCUS can be used to rapidly assess for signs of early tamponade.
If there is any question, consider expert consultation immediately and/or consider emergent pericardiocentesis depending on the clinical situation.
Pericardial Effusions —
Evaluate for pericardial effusions in multiple views starting with the PSL.
Should see descending aorta in PSL as a landmark. If not visualized, adjust depth.
Pericardial effusions will be above the descending aorta, pleural effusions will be next to it.
Acuity matters more than size. Slow growing effusions can be tolerated well to large sizes. Tamponade occurs due to a mismatch between rate of accumulation and pericardial stiffness/compliance.
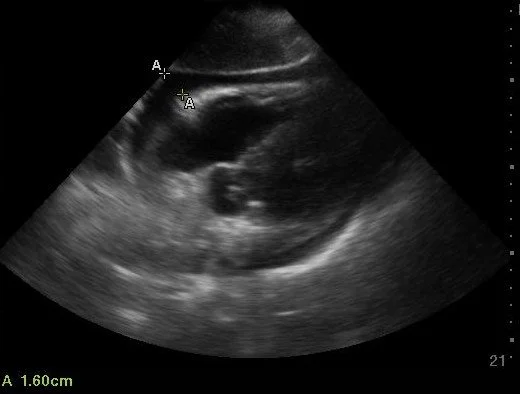
Differentiating fat pad from pericardial effusions —
Pericardial fat pad — noncircumferential accumulation of heterogeneous material that moves in concert with the heart, restricted to the region around the right heart.
Pericardial effusions — anechoic or mixed echotexture that displaces with heart movement. Hemorrhagic pericardial effusions may appear like fat pads and be difficult to distinguish.
Prominent pericardial fat pad (with trace effusion)
Pericardial fat pad and pericardial effusion — note the pericardial fat pad moving in concert with the right heart while the pericardial effusion is circumferential.
Hemorrhagic pericardial effusion — note how the complex fluid goes beyond the right heart and is circumferential.
Size Evaluation —
Pericardial effusions are measured by using the a linear measurement largest pocket at end diastole.
The most common system uses the following measurements:
| Measurement (cm) | Qualitative | Volume (approximate in mL) |
|---|---|---|
| Only visible in systole | Trace or Trivial | <50 |
| 0-1 | Small | 50-100 |
| 1-2 | Moderate | 100-500 |
| >2 | Large | >500 |
Trace or trivial pericardial effusions may be physiologic, functioning as a lubricant for heart motion.
There is no real agreement on size parameters for pericardial effusions and some argue for volumetric measurements due to the asymmetrical nature of pericardial effusions.
Trace / Trivial
Small
Moderate
Large
Extra Large Pericardial Effusion
Measurements —
Measure multiple areas if multiple areas visible and evaluate in other views as well.
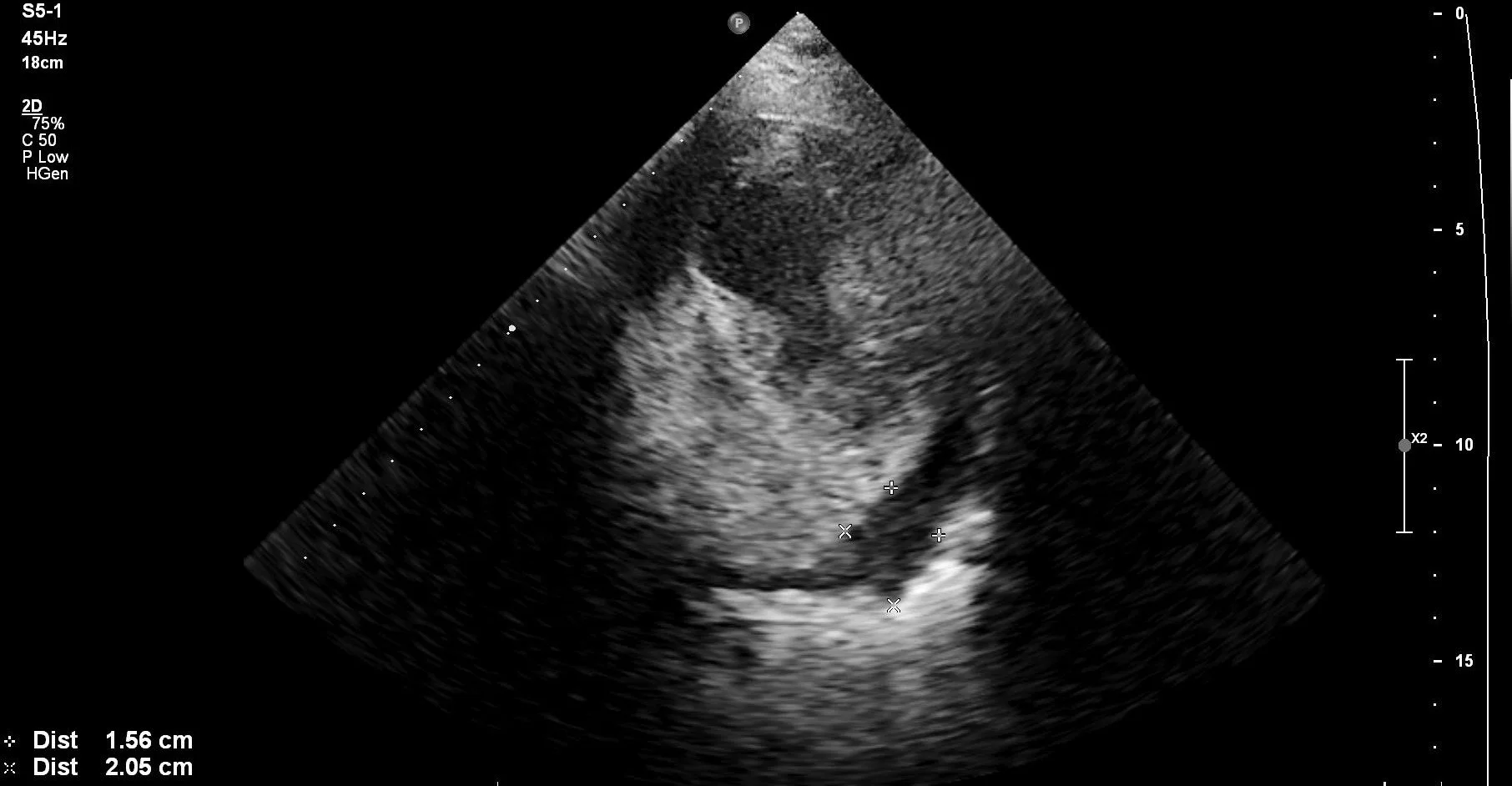
PSS pericardial effusion measurement
SX pericardial effusion measurement
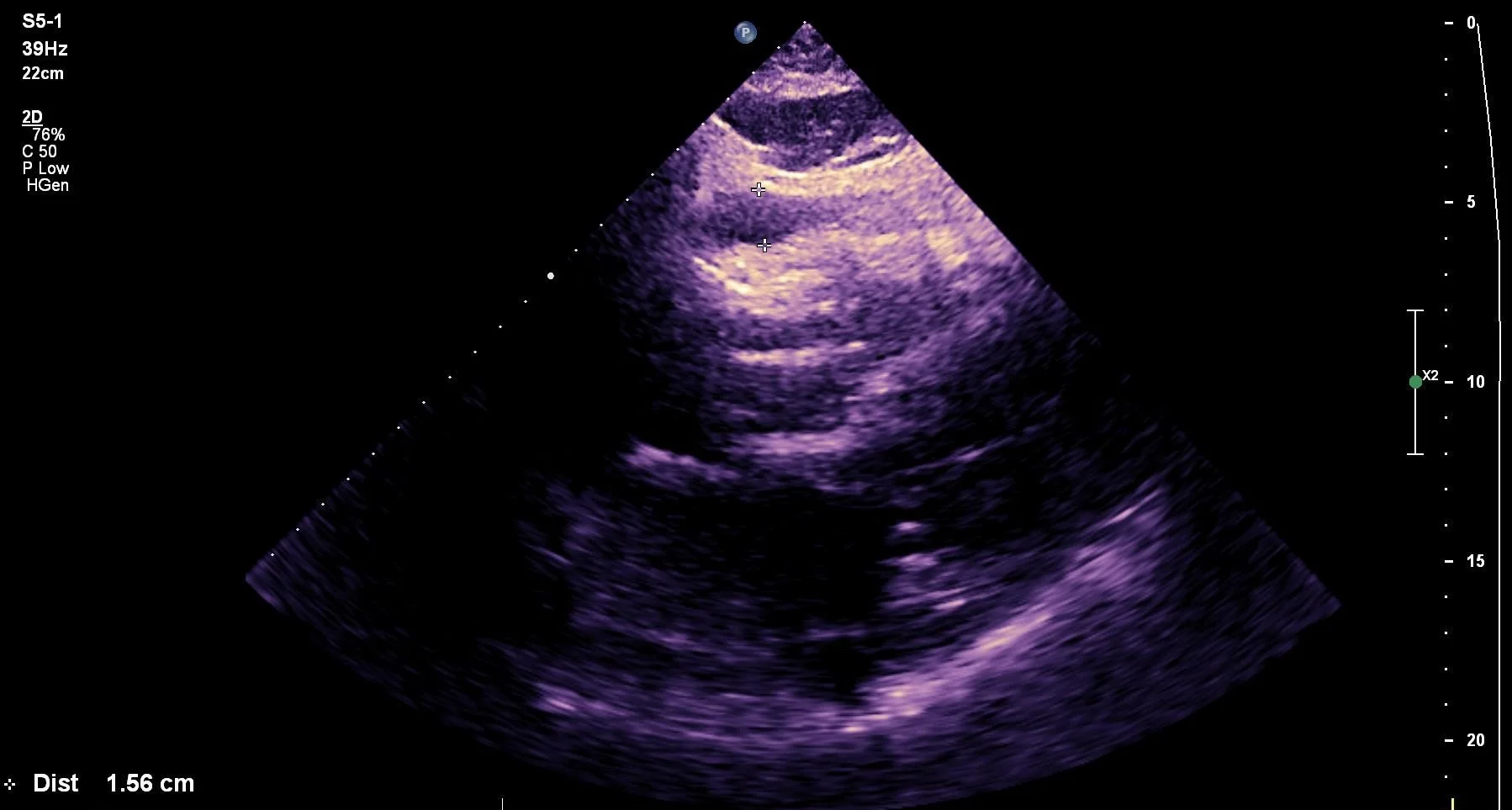
SX pericardial effusion measurement
Diagnosing Tamponade
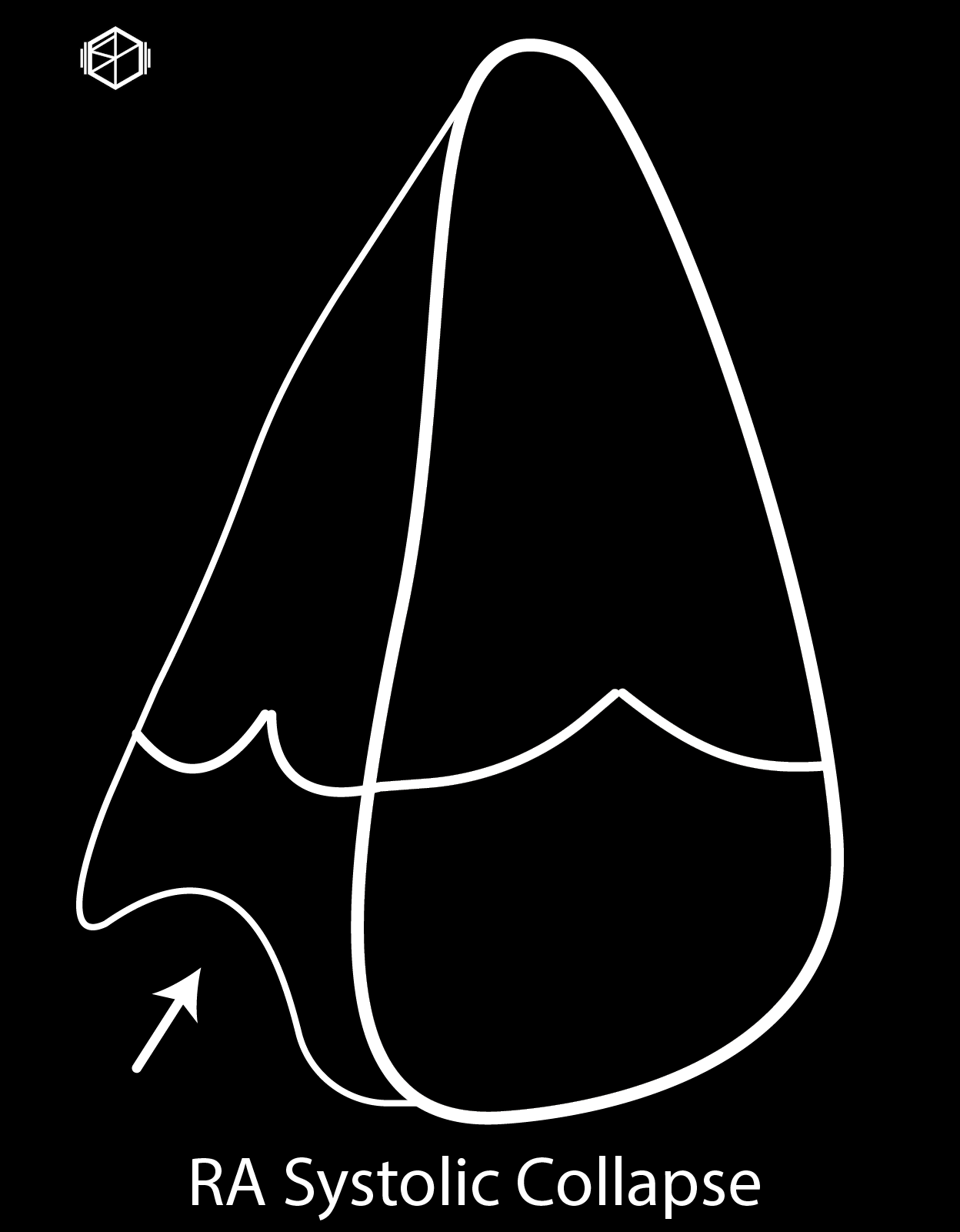
Right Atrial Systolic Collapse —
RA pressure is the lowest during systole/late diastole during atrial relaxation. Pressure from external pericardial effusion can cause collapse of the RA at this time.
Use slow motion / cine to view clips to see when valve is closed to evaluate for RA collapse.
Earliest sign of tamponade.
Sensitivity — moderate to high
Specificity — moderate to high
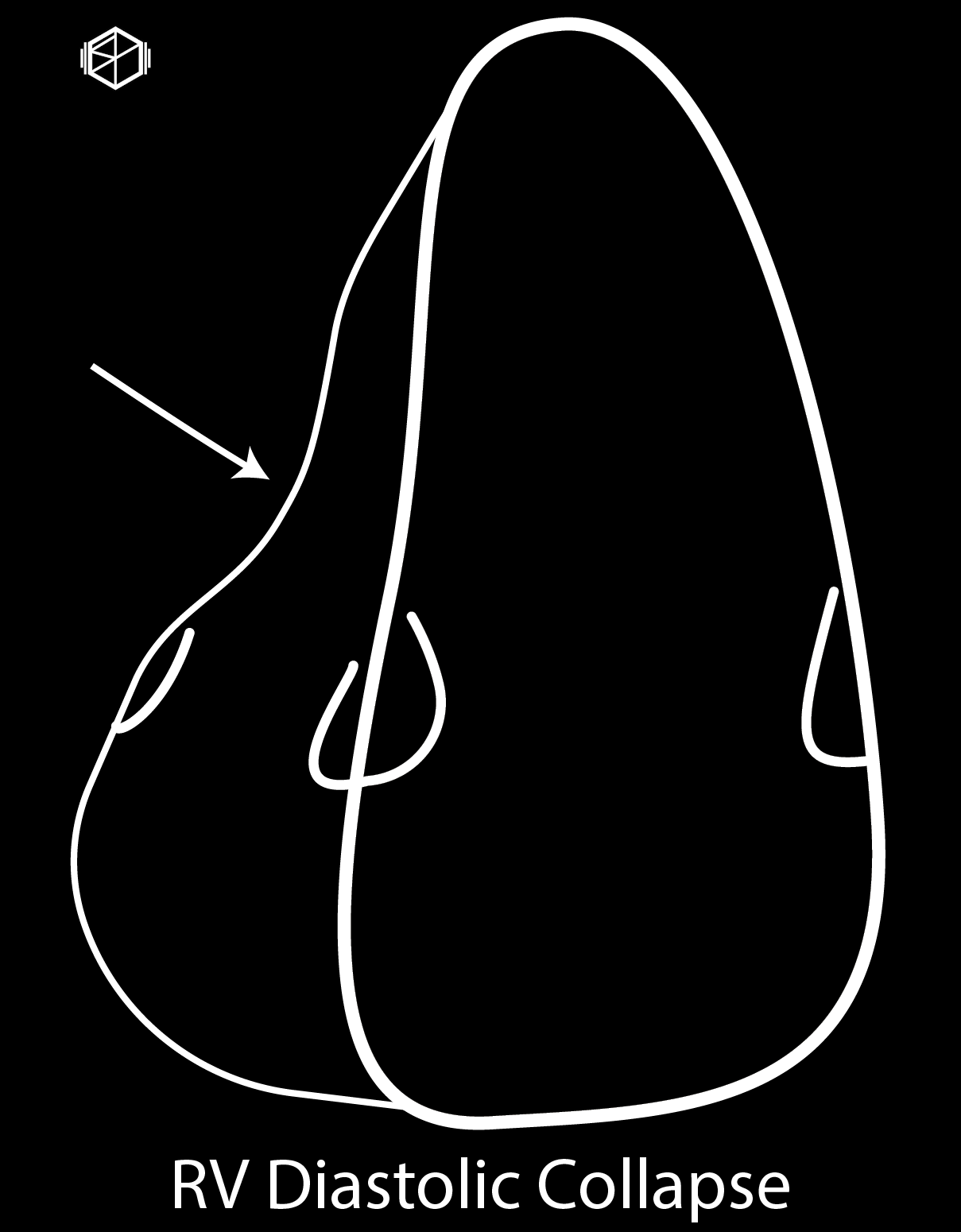
Right Ventricular Diastolic Collapse —
RV is thinner walled, lower pressure than LV. Lowest pressure during early diastole. Intrapericardial pressure can can exceed intraventricular pressure at this time causing bowing.
Use slow motion / cine to view clips to see when valve is open to evaluate for RV collapse.
Can be visualized in all cardiac views.
Sensitivity — moderate
Specificity — moderate to high (generally considered to be on the higher end).
Pathologies in which RV pressures are elevated at baseline decrease the risk of diastolic RV collapse.
Pulmonary HTN, acute or chronic cor pulmonale, RV hypertrophy/failure, positive pressure ventilation
Dependent on volume — hypovolemia higher risk.
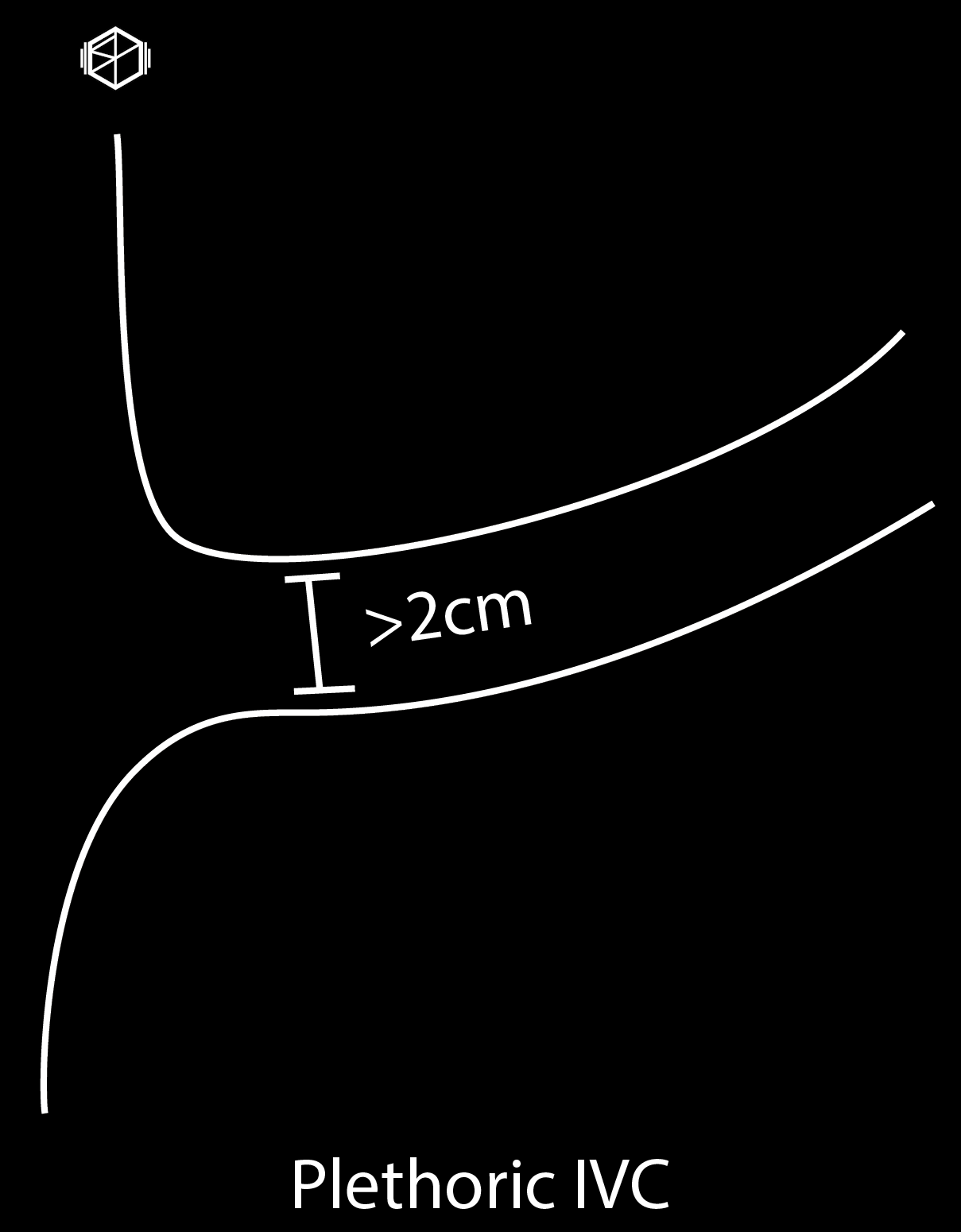
Plethoric IVC with minimal respiratory variation —
Elevated intrapericardial pressures lead to decreased preload.
Sensitivity — high (most sensitive)
May be absent in loculated pericardial effusions post trauma/cardiac surgery or low pressure tamponade.
Specificity — poor; can be caused by a variety of other pathologies including CHF, pulmonary embolism, tricuspid regurgitation.
High negative predictive value — if the IVC is not plethoric the patient is less likely to have clinically significant tamponade.
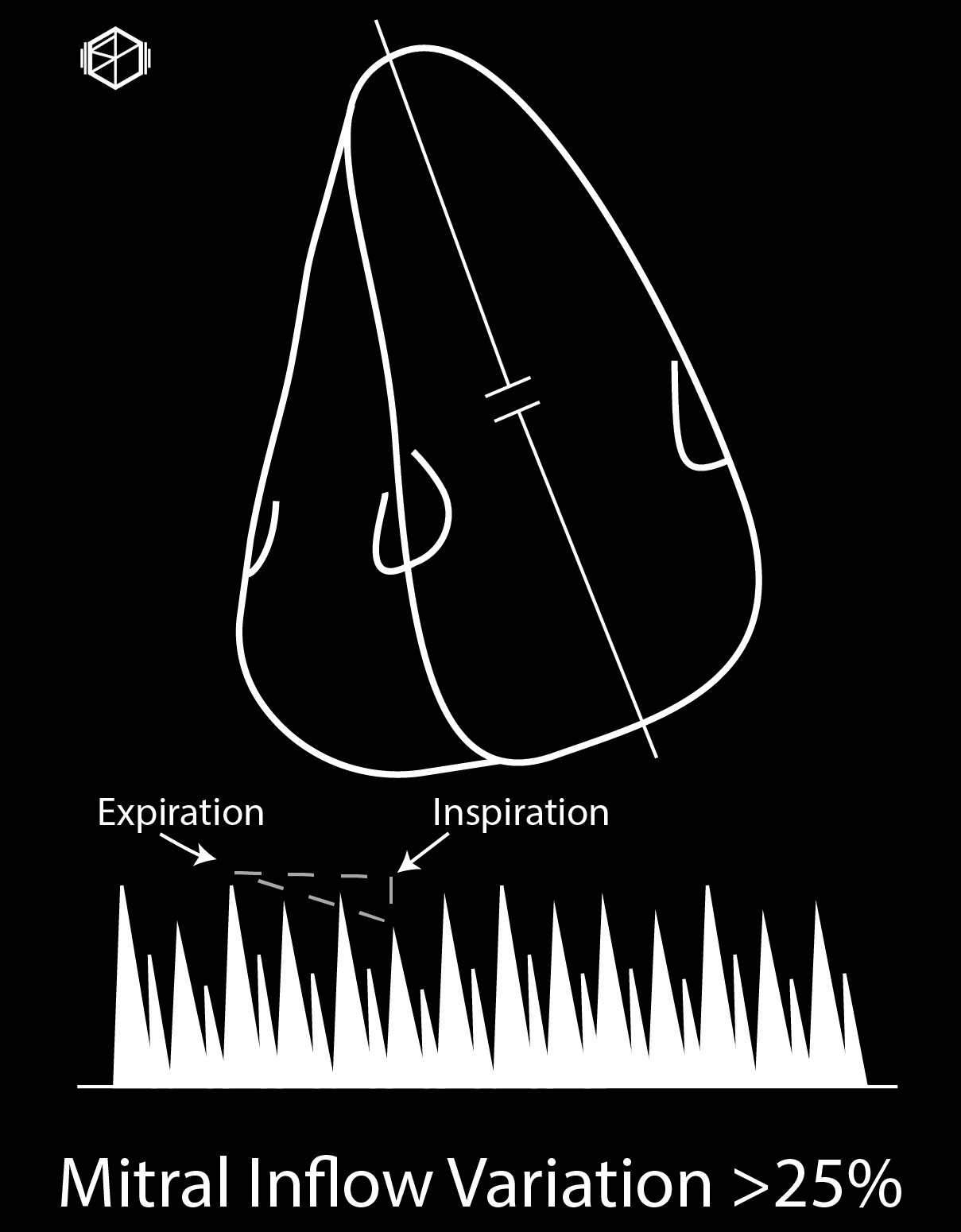
Mitral Inflow Variation >25% —
More advanced evaluation using doppler studies, not always necessary for POCUS evaluations.
Pulse wave doppler just past the tip of the mitral valve.
Principle of ventricular interdependence. Similar to pulsus paradoxus.
Measure difference between tallest E wave and lowest E wave and if Δ >25% indicates possible tamponade.
Limitations —
Operator dependent
Patient positioning
Sample volume issues
May not occur in patients with severe pulmonary hypertension, hypervolemia, ventricular dysfunction/hypertrophy, positive pressure ventilation.
Lower specificity — may occur in patients with pulmonary embolism, severe COPD, severe shortness of breath.
Other findings —
Tricuspid inflow variation > 40% — similar to above except through tricuspid valve.
Left sided tamponade (atypical, rare):
Loculated pericardial effusions may cause localized tamponade and lead to left sided tamponade. Post-cardiac surgery, malignancy, and rheumatological diseases pose risk for complex pericardial effusions.
May see left ventricular tamponade in patients with significantly high right sided pressures — pulmonary hypertension, cor pulmonale from pulmonary embolism.