
POCUS Echocardiography
General notes —
Evaluation for right heart strain is very important for critical diagnoses such as pulmonary embolism, pulmonary hypertension, and right heart failure.
Basic evaluation right heart strain includes assessment for —
A dilated right ventricle (>2/3rd the size of the LV)
McConnell’s sign
D-sign, abnormal septal displacement (paradoxical septal motion)
Tricuspid regurgitation (qualitative)
Right ventricular systolic dysfunction — as measured by tricuspid annular planar systolic excursion < 1.7cm (TAPSE)
Plethoric IVC
A dilated right ventricle —
The normal size of the right ventricle is 2/3rd the size of the right ventricle.
The AP4 is generally the best view to assess RV size; however, can also look at the PSS.
Subxiphoid is the preferred view to assess for RV wall thickness to assess for RV hypertrophy (20620859).
The right atrium and the right ventricle have some of the lowest pressures in the heart.
Anything that causes increased pulmonary vascular resistance (eg, PE) will cause an increase in right ventricular afterload. The RV is relatively thin walled and thus will dilate in response to the increased pressure.
For pulmonary embolism, the presence of a dilated right ventricle has a lower sensitivity, but high specificity (24075286).
McConnell sign —
Seen in the AP4 view.
Described as regional hypokinesis of the RV-mid free wall and hyperkinesis of the RV apex, or RV hypokinesis with apical sparing (15664548).
The right ventricle contracts longitudinally (much like a trap door), while the left ventricle contracts concentrically. Increased pulmonary vascular resistance leads to decreased RV lateral contractility while the apex is spared.
Considered a specific, but not a sensitive sign for PE (15664548, 28495379, 31056367, 31562679).
D-sign (abnormal septal displacement) —
D-sign visualized in the PSS.
The D-sign is a good indicator of either RV volume overload or RV pressure overload (16543596).
With a normal heart, the LV should appear circular both in systole and diastole.
With RV volume overload, the LV deforms into a D-shape during end-diastole, but remains circular during systole.
RV volume overload may occur due to multiple reasons, most commonly, aggressive volume resuscitation, severe tricuspid regurgitation, decompensated heart failure.
With RV pressure overload, LV is D-shaped throughout systole and diastole due to significantly elevated RV afterload.
RV pressure overload may occur due to multiple reasons, the goal is to find a cause. The potential causes of RV pressure overload include — massive pulmonary embolism, left sided heart failure, pulmonary hypertension, chronic right sided heart failure, ARDS.
RV pressure overload — note how the LV never really turns back to a circular shape (pulmonary embolism).
RV pressure overload — notice how the septum stays flattened during both systole and diastole (pulmonary hypertension).
RV volume overload — note how the LV turns into a circular shape (chronic right heart failure with fluid overload).
RV volume overload — subtle D-sign (septic shock leading to ARDS with increased PVR leading to right heart volume overload).
Abnormal septal deviation —
Can be visualized in any view. Similar to above, just visible in other views.
May occur for multiple reasons as noted above including high pulmonary pressures or volume overload. May also occur in early systole with left bundle branch block although this will be obvious from the ECG (34760507).
Septal displacement toward LV during diastole — RV volume overload.
Septal displacement toward LV during diastole — RV volume overload.
Septal displacement — RV pressure overload (PE)
Septal displacement toward RV — RV pressure overload (PE)
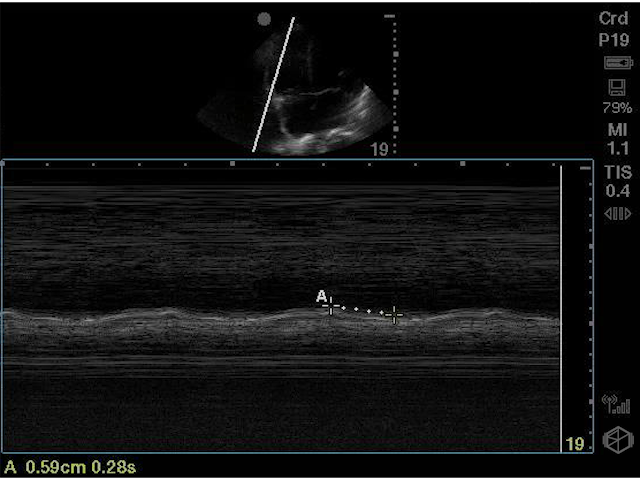
Tricuspid annular plane systolic excursion (TAPSE) —
TAPSE is a marker for RV systolic function. It reflects the longitudinal contraction of the RV.
Performed by getting an A4C view and placing the M-mode line over the lateral wall of the RV at the tricuspid annulus. Align the beam toward the motion of the tricuspid annulus. Press the M-mode button again. A curved tracing will be obtained. Measure the peak to trough.
A normal TAPSE is >1.7cm (25559473).
Prognostically — a decreased TAPSE in PE is independently predictive of 30-day mortality (31735658, 24412192, 24766779, 27695491, 29375106).
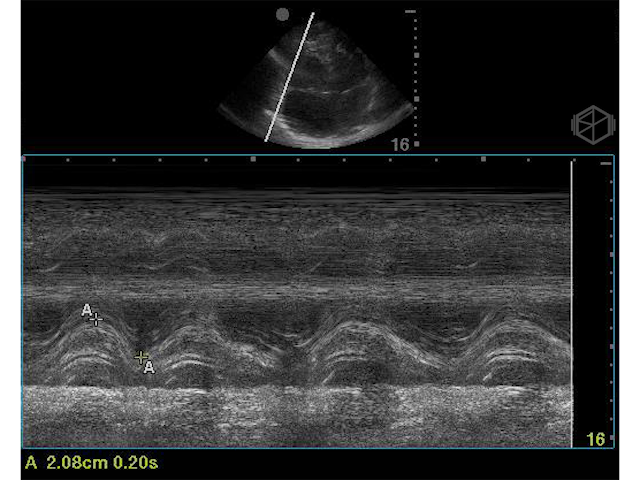
Normal TAPSE
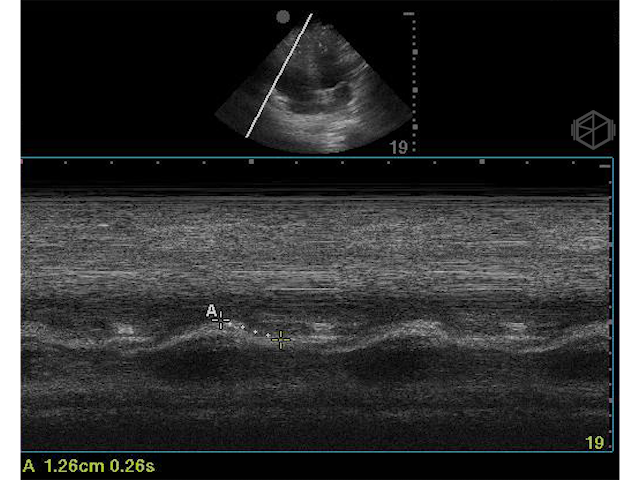
Reduced TAPSE
Significantly reduced TAPSE
Tricuspid regurgitation (qualitative) —
Apical 4 chamber or PSAX view at the level of the tricuspid valve.
Occurs due to dilatation of the right ventricle which leads to dilatation of the tricuspid valve annulus which in turn leads to coaptation of the tricuspid valve leaflets leading to tricuspid regurgitation (31185724).
Basic qualitative assessment — visualization of the tricuspid jet hitting the backwall of the RA is indicative of severe tricuspid regurgitation.
Again, high specificity, lower sensitivity (28495379).
Prognostically, patients with significant TR and RV systolic dysfunction (low TAPSE) have worse outcomes despite RV size (31185724).
Moderate to Severe Tricuspid Regurgitation
Moderate to Severe Tricuspid Regurgitation
Severe Tricuspid Regurgiation
Plethoric IVC —
The IVC can be plethoric for many reasons including right heart strain.
IVC can be dilated in patients on positive-pressure ventilation.
In patients with indeterminates IVC diameter a value of 8mmHg can be used (25559473).
RAP and CVP are interchangeable as long as there is no IVC obstruction (23860098).
| IVC Size | Collapsibility | Right Atrial Pressure (RAP) | |
|---|---|---|---|
| Hypovolemic | <2.1cm | Flat IVC | Hypovolemic patient |
| Normal | <2.1cm | >50% (Normal) | 3 mmHg |
| Intermediate | <2.1cm | <50% (Abnormal) | 8 mmHg |
| >2.1cm | >50% (Abnormal) | 8 mmHg | |
| High | >2.1cm | <50% (Abnormal) | 15 mmHg |